60 y old male patient with shortness of breath and decreased urine output
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings investigations and come up with diagnosis and treatment plan.
A 60 year old male who is a resident of suryapet ,farmer by occupation came to opd with
Chief Complaints of :-
- Pedal edema since 3 months
- Shortness of breath Since 20 days
- Decreased urine output since 15 days
- Weakness of lower limbs since 4 days
History of presenting illness :-
The patient was apparently asymptomatic 3 months back when he noticed bilateral pedal edema initially extending upto the ankle and gradually progressed upto thighs which worsened during last 15 days.
- Decreased urine output since 15 days, not associated with frequency, urgency or burning micturation.
- Grade 3 shortness of breath, no aggravating and relieving factors.
- Fever since 15 days intermittent associated with chills and
rigors.
Series of events :-
History of trauma by fall from tree 25 years back for which he used NSAIDS for 4/5 yrs.
7 years back when patient was undergoing hydrocele surgery he was diagnosed with ckd accidentally for which he got treated by dailysis initially and then he started using medications and was apparently well till 3 months back.
3 months back patient developed bilateral pedal edema, facial puffiness for the first time and shortness of breath so he visited local hospital and they referred to our hospital for dailysis.
Since then patient was coming here regularly twice a weak for dialysis .
After his last dialysis session he went back home and he developed discomfort in chest and weakness of limbs . Patient also had few episodes of altered sensorium in between which was associated with fever and chills .So he was brought to hospital again.
Past history :
He is known case of hypertension since 6 months and is on medication.
Not a known case of asthma,diabetesmellitus,epilepsy,tuberculosis.
Personal history:-
Mixed diet,normal bowel movements,decreased urine output since 15 days .
Addictions :- consumed alcohol for 20 years every 3/4 days
Consumed toddy everyday for 40 years.
Daily routine:-
Before 3 years :-
Wakes up at 5 am and goes to field and toddy trees
Breakfast at 9 am -rice
Afternoon- lunch 12 pm
Evening drinks toddy
And dinner by 9 pm and sleep
Now :
Wake up at 8 am
Breakfast at 9 am
Skips lunch and dinner at 8 pm
He is not going to work,not as active as in the past.
Family history:-
Father had hypertension
General Examination:
- Patient is conscious, coherent,cooperative.
-Moderately built and nourished.
-pallor present

Pedal edema -


- clubbing is seen

- no signs of icterus , generalized lymphadenopathy.
-bilateral pedal edema.( Pitting)
Vitals:-
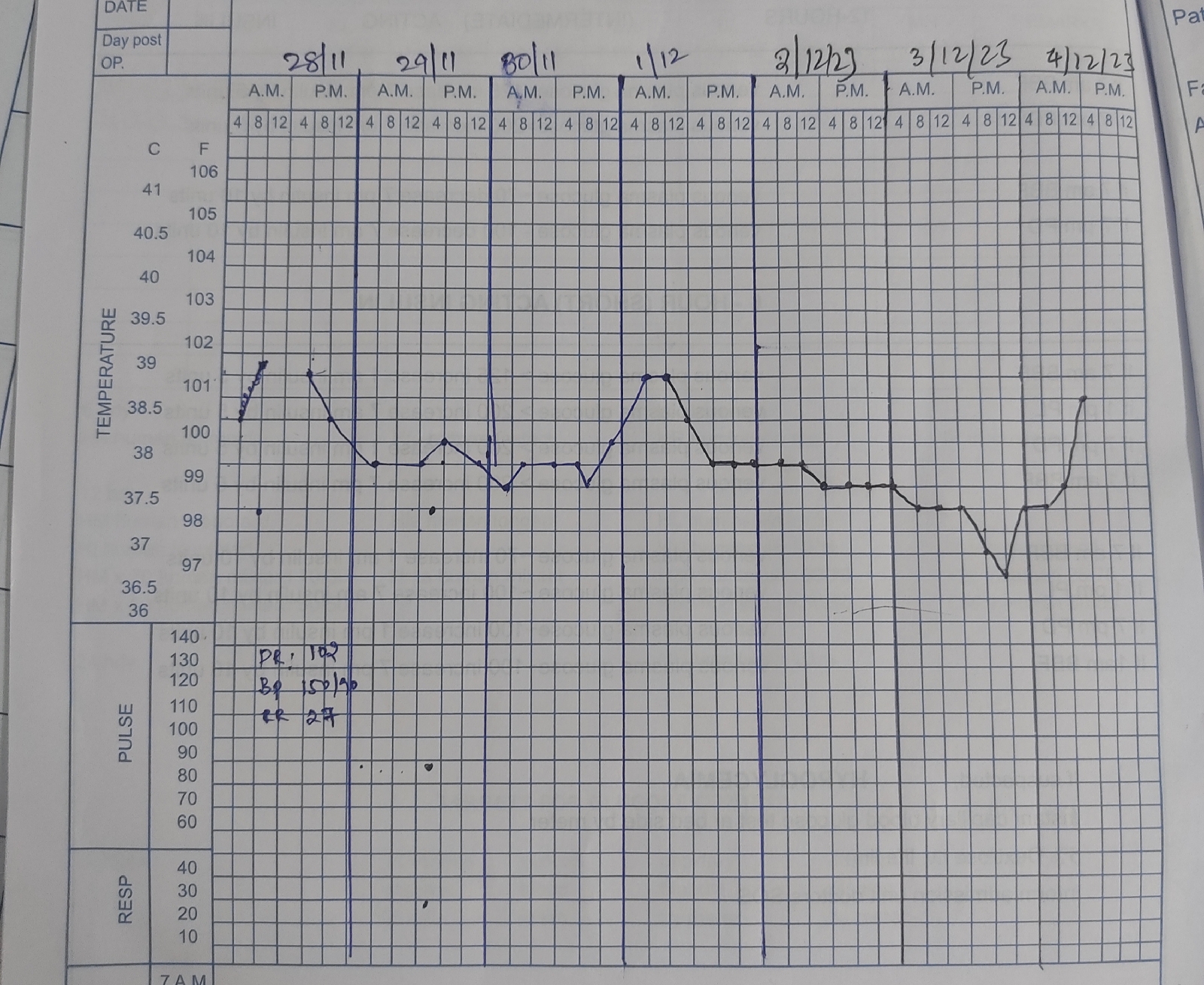
Temp:99.1°F
PR: 98
Rr: 29/ min
Bp:100/80 mm Hg.
Spo2: 84%
GRBS:124 mg/dl
-Systemic examination:-
Cardiovascular System:-
On Inspection:-
Chest wall is bilaterally symmetrical.
No precordial bulge is seen
No spine deformity
No precordial prominence
No scars and distended veins
No Apical Impusle
On Palpation:-
No local rise of temperature and tenderness
Apex beat -felt in the left 5th intercoastal space in the mid clavicular line
No cardiovascular pulsation like no thrills and rubs felt
On Auscaltation-
Mitral area apex -S1 S2heard;no murmur
Tricuspid area - S1 S2 heard;no murmur
Aortic area - S1 S2 heard;no murmur
Pulmonary area- S1 S2 heard;no murmur
Respiratory system:
-Position of trachea central.
- Bilateral airway entry present.
-Dyspnea present
- no wheeze.
Abdomen:
-Scapoid
-No tenderness
-No palpable mass
-Spleen : not palpable
-liver : not palpable.
CNS examination:
Higher mental functions are intact
Cranial nerves are intact
Motor system:
Nutrition:
Right Left
Mid arm 25cm. 25 cm
Fore arm. 18 cm. 18 cm
Mid thigh. 37 cm. 37 cm
Mid leg 27 cm. 27 cm
Tone
R. L
Upper limb Hypertonia Hypertonia
Lower limb. Hypertonia Hypertonia
Power R. L
Upperlimb 4/5 4/5
Lowerlimb 3/5 3/5
Reflexes :
Superficial :-
Corneal present
Conjunctival present
Abdominal present
Plantar present
Deep:-
Reflexes are absent
Sensory system:-
TEST RIGHT LEFT
I – SPINOTHALAMIC
1. Crude touch. N. N
2. Pain. N. N
3. Temperature. N. N
II – POSTERIOR COLUMN
1. Fine touch. N. N
2. Vibration. Unable to perform
3. Position sense. 3/10. 4/10
III – CORTICAL
1. Two point discrimination. N. N
2. Tactile localisation. N. N
3.Stereognosis. N. N
Cerebellar signs :-
No nystagmus ,no pendular knee jerk,no tremors
Coordination:-
Finger nose test : abnormal
Heel knee test : abnormal
Gait:- patient is walking with support by attenders and by bending forward
Investigations:









Provisional diagnosis :
Chronic kidney disease on maintenance hemodialysis with anemia of chronic disease with hypertension.
Treatment
Inj PIPTAZ : 2.25 gm I.v twice a day.
Inj LASIX : 40 mg Iv twice a day
Inj NEOMAL : 14mg IV sos
Tab : Oral NODOSIS 500 mg twice a day
Tab: Oral SHELCAL 50 mg twice a day
Tab : oral ECOSPRIN 50mg H/S
Tab OROFER once a day
Tab : DOLO 650 mg QID.
On 28 /11/23
Patient was on salt restriction < 1.5 g / day
Patient was on fluid restriction <1.5l per day
Inj : PIPTAZ 2.25 gm iv /tid
Inj LASIX 40 mg iv /bid
Inj MEOMOL 14 mg iv sos if temp >101
Tab : ECOSPRIN 50mg H/S
Tab : OROFER once a day
Tab DOLO 650 mg every 6 hourly
Tab NODOSIS 500 mg PO /BD
Tab SHELCALT 500 mg /BD.
On 29/11/23
TAB. LINOD 10mg twice a day.
Inj LASIX : 40 mg Iv twice a day
Tab : Oral NODOSIS 500 mg twice a day
Tab: Oral SHELCAL 500 mg twice a day
Inj.EPO 4000 IU ,SC once weekly
Tab : oral ECOSPRIN 75mg H/S
Inj NEOMAL : 14mg IV sos
Tab : DOLO 650 mg QID
Inj PIPTAZ : 2.25 gm I.v thirice a day.
On 30 /11/23
Treatment
Inj PIPTAZ : 2.25 gm I.v twice a day.
Inj LASIX : 40 mg Iv twice a day
Inj NEOMAL : 14mg IV sos
Tab : Oral NODOSIS 500 mg twice a day
Tab: Oral SHELCAL 50 mg twice a day
Tab : oral ECOSPRIN 50mg H/S
Tab OROFER once a day
Tab : DOLO 650 mg QID
Intermittent CPAP
Oxygen supplementation 1-2



Comments
Post a Comment